
Contact Us
Following major changes in the biomarkers available for diagnosis, criteria for acute myocardial infarction have been revised.
The current international consensus definition states that the term ‘acute myocardial infarction’ (AMI) should be used when there is evidence of myocardial necrosis in a clinical setting consistent with myocardial ischaemia. Hence ‘acute myocardial infarction’ (AMI) should be used when there is evidence of myocardial necrosis in a clinical setting consistent with myocardial ischaemia.. Under these conditions, any one of the criteria described below meets the diagnosis for spontaneous myocardial infarction.
The current international consensus definition states that the term ‘acute myocardial infarction’ (AMI) should be used when there is evidence of myocardial necrosis in a clinical setting consistent with myocardial ischaemia. Hence ‘acute myocardial infarction’ (AMI) should be used when there is evidence of myocardial necrosis in a clinical setting consistent with myocardial ischaemia.. Under these conditions, any one of the criteria described below meets the diagnosis for spontaneous myocardial infarction.
- Detection of rise and/or fall of cardiac biomarker values (preferably troponin) with at least one value above the 99th percentile of the upper reference limit and with at least one of the following:
- Symptoms of ischaemia
- New or presumably new significant ST-T changes or new LBBB
- Development of pathological Q waves in the ECG
- Imaging evidence of new loss of viable myocardium, or new regional wall motion abnormality
- Identification of an intracoronary thrombus by angiography or autopsy
A history of chest pain lasting for 20 min or more, not responding to nitroglycerine. Important clues are a history of coronary artery disease (CAD) and radiation of the pain to the neck, lower jaw or left arm.
The pain may not be severe. Some patients present with less-typical symptoms, such as nausea/vomiting, shortness of breath, fatigue, palpitations or syncope. These patients tend to present later, are more likely to be women, diabetic or elderly patients, and less frequently receive reperfusion therapy and other evidence-based therapies than patients with a typical chest pain presentation. Registries show that up to 30% of patients with STEMI (ST elevation MI) present with atypical symptoms.
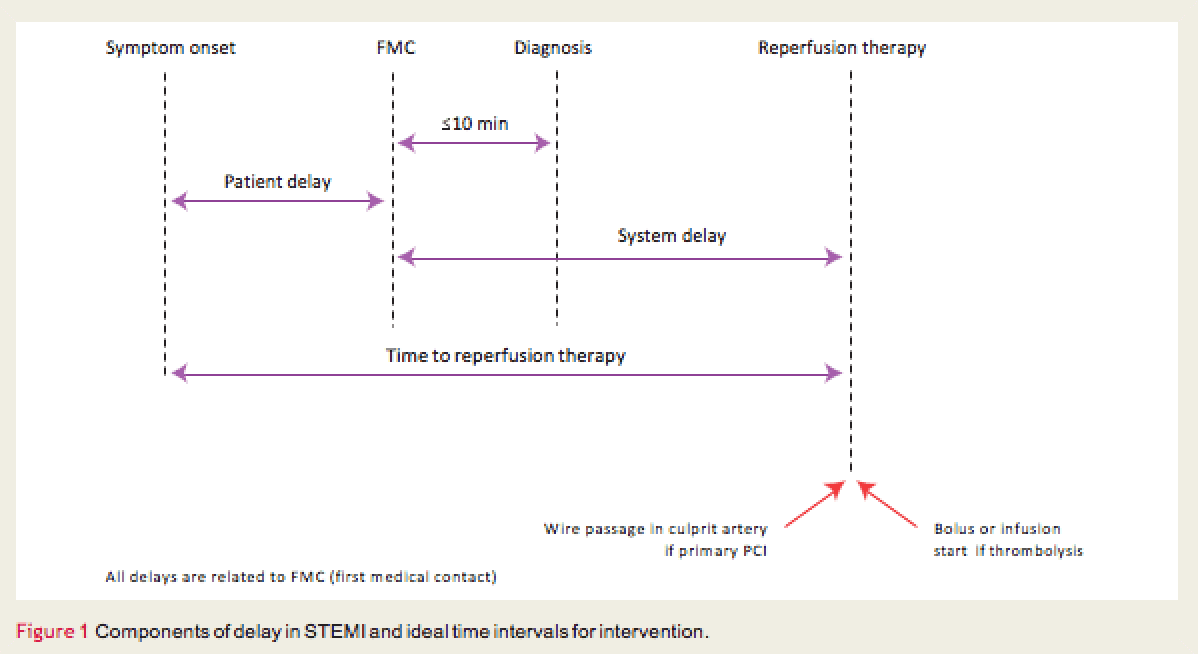
Timely diagnosis of STEMI is key to successful management.
ECG monitoring should be initiated as soon as possible in all patients with suspected STEMI to detect life-threatening arrhyth-mias and allow prompt defibrillation if indicated. A 12-lead ECG should be obtained and interpreted as soon as possible.
Prevention of delays is critical in STEMI for two reasons:
Minimising delays is associated with improved outcome
European Heart Journal (2012) 33, 2569–2619.
Scan the QR code to book a consultation with Dr Forbat, or click here to send a message
The pain may not be severe. Some patients present with less-typical symptoms, such as nausea/vomiting, shortness of breath, fatigue, palpitations or syncope. These patients tend to present later, are more likely to be women, diabetic or elderly patients, and less frequently receive reperfusion therapy and other evidence-based therapies than patients with a typical chest pain presentation. Registries show that up to 30% of patients with STEMI (ST elevation MI) present with atypical symptoms.
Timely diagnosis of STEMI is key to successful management.
ECG monitoring should be initiated as soon as possible in all patients with suspected STEMI to detect life-threatening arrhyth-mias and allow prompt defibrillation if indicated. A 12-lead ECG should be obtained and interpreted as soon as possible.
Prevention of delays is critical in STEMI for two reasons:
- The most critical time of an acute myocardial infarction is the very early phase, during which the patient is often in severe pain and liable to cardiac arrest.
- A defibrillator must be made available to the patient with suspected acute myocardial infarction as soon as possible, for immediate defibrillation if needed.
Minimising delays is associated with improved outcome
European Heart Journal (2012) 33, 2569–2619.

Litfield House Medical Centre
1 Litfield Place Clifton Down
Bristol
BS8 3LS
Visit https://www.litfieldhouse.co.uk/consultant/lance-forbat/
also on Doctify https://www.doctify.com/uk/specialist/dr-lance-forbat#about
WHO IS "HEART2HEART" DOCTOR?
Read more
Dr. Lance Forbat brings innovative cardiology services using new technologies and has a special interest in telemedicine.
Your symptoms may not be a heart attack but don't ignore them. Heart2Heart Dr. offers a personal service. Request a home visit. I perform 12 lead ECG, ECHO, , fit a 24HrBP and offer a 2 week Zio-Patch for ambulatory monitoring. Telemedicine (see: https://www.youtube.com/watch?v=0Mi3BTmJ2E8&t=18) with Careportal enables Dr Forbat to diagnose, monitor & treat your heart & related conditions.. Have for you or a loved one.
Dr. Forbat is MD of MTT (Cardiology) Ltd and has monitored over a 100 patients to date. He is currently able monitor up to 8 patients daily. potential .
Your symptoms may not be a heart attack but don't ignore them. Heart2Heart Dr. offers a personal service. Request a home visit. I perform 12 lead ECG, ECHO, , fit a 24HrBP and offer a 2 week Zio-Patch for ambulatory monitoring. Telemedicine (see: https://www.youtube.com/watch?v=0Mi3BTmJ2E8&t=18) with Careportal enables Dr Forbat to diagnose, monitor & treat your heart & related conditions.. Have for you or a loved one.
Dr. Forbat is MD of MTT (Cardiology) Ltd and has monitored over a 100 patients to date. He is currently able monitor up to 8 patients daily. potential .
Contact Us
COME AND VISIT MY CLINIC
Home visits open
Contact Olivia Forbat on 07789 174044
or e-mail
omf.1@live.com
lance.forbat@privatecardiologyservices.com
1 Clifton Down
Clifton
Bristol
BS8 3LR
Your Heart2Heart Doctor
Dr Forbat qualified from St. Thomas’ Hospital Medical School, University of London gaining a BSc Physiology with 1st Class Honours 1977 and MBBS 1980.
He returned St. Thomas’ as a British Heart Foundation Junior Research Fellow in 1987. He was awarded his MD in 1994.
He was appointed as Consultant Cardiologist at West Cumberland Hospital and Honorary Consultant Cardiologist South Cleveland in 1995.
He has brought new services to several other units and led three departments.
Previoiusly an honorary consultant at University Hospitals Coventry and Warwikshire NHS Trust he has become a fully independant provider, working as required as a Locum Consultant around the UK
Read more
He returned St. Thomas’ as a British Heart Foundation Junior Research Fellow in 1987. He was awarded his MD in 1994.
He was appointed as Consultant Cardiologist at West Cumberland Hospital and Honorary Consultant Cardiologist South Cleveland in 1995.
He has brought new services to several other units and led three departments.
Previoiusly an honorary consultant at University Hospitals Coventry and Warwikshire NHS Trust he has become a fully independant provider, working as required as a Locum Consultant around the UK